It’s been quiet around here, quieter than I’d planned but so much of this summer has not exactly gone according to plan, so I’m trying to roll with that.
Since we last spoke about Lyme disease and its co-infections, we’ve had weeks of renovations, moving, unpacking, some health crises, etc., but we’re finally getting settled.
There is a whole lot of “new”—new town, new house, new physical therapist, new job responsibilities, and more, right now.
But in spite of the long (hot) hours working on the house, the juggling, and the overall upheaval of the past couple months, it’s beginning to feel like home. My office is unpacked, and my desk overlooks a window with a stream of sunshine and a rather bucolic view. My daughter knows where all her toys and books belong, and loves her yard and her porch. “Hello, new house!” she exclaims when we pull into the neeighborhood. “Goodbye new house! Goodbye flowers and trees and water table!” she calls merrily when we leave.
And it feels like more than simply new; it feels like the beginning of something better. There is a lot say about that, and about getting a new physical therapist, and about juggling work and illness, and about parenting an almost-two-year-old, and so much other stuff.
(And I just got my copy edits on my manuscript back—I have an ISBN, people. This is getting real!)
Now that my physical space is sorted a bit, I’m finding my mental space is realigning too, and I can better focus on this virtual space. I’m working on a bunch of posts, and more long-term, working on a new look and feel.
For a long time, I’ve struggled to regain my rhythm. Life needed a reset button, and I think I found it.
Last week, WBUR, the local NPR station, ran a week-long look at Lyme disease and chronic Lyme disease. The controversy over chronic Lyme disease (and specifically, how social media and the Internet have influenced patient advocacy and Lyme literacy) is something I explore in a later section of my forthcoming book, so I was interested in seeing mainstream media offer a sustained look at the issue. I know several people who have suffered from Lyme disease and chronic Lyme, including Jennifer Crystal, a writer and grad student at my graduate school alma mater, Emerson College. I spoke with Jennifer at length when I interviewed her for my book, and I checked in with her in the wake of this recent media coverage.
Even if you haven’t been touched by Lyme personally, Jennifer’s diagnostic journey and her thoughts on ignorance and fear will resonate with anyone who has struggled to receive a correct diagnosis.
1. I know your journey to diagnosis was long and complicated. While I share the longer version in my book, can you give readers a brief synopsis of your story? Would you agree it shares similarities with Barbara McLeod’s Lyme story, which WBUR reported on last week, and which received a lot of interest and feedback?
My story is very similar to Barbara’s, in that we both got sick when we were young, otherwise energetic and eager professionals, and we both struggled for too long to maintain that identity while mysterious symptoms ate away at our lives. Like Barbara, my tick-borne illnesses went undiagnosed for a long time, and I was repeatedly turned away by doctors who thought I was stressed, run down or depressed.
I was bitten by a tick in 1997 while working at a summer camp in Maine, but my waxing and waning flu-like symptoms did not get properly diagnosed until 2005. By that time the Lyme bacteria, as well as the co-infections ehrlichia and babesia, had spread to every system of my body and crossed the blood-brain barrier. I wrestled with severe physical and neurological symptoms that left me bedridden and unable to work or care for myself. It took many years of treatment, including intravenous antibiotics and strong anti-malarial medication, to get me back on my feet. I am much, much better than I was several years ago, but I still live with limitations today and still take medication to help maintain a certain level of health.
2. Much of the current debate centers on chronic Lyme. Again, I know this is a complicated situation, but can you briefly discuss why you think there is such resistance to the existence of chronic Lyme from some factions of the medical establishment? I think the resistance comes down to two factors: ignorance and fear.
The Infectious Disease Society of America mandates that all cases of Lyme disease can be treated with 28 days of antibiotics. This is true for cases that are found and diagnosed right away. However, all too often, Lyme disease goes undiagnosed and untreated, mistaken for other conditions like chronic fatigue syndrome, MS, arthritis or lupus. Some doctors only know to look for a bull’s eye rash, which manifests in less than 50% of cases of Lyme disease. To make matters worse, Lyme disease testing is not reliable and not always accurate, so there are a lot of false negative tests. For these reasons, the Lyme bacteria can be left to replicate for months or even years, wreaking havoc on the whole body. Any infection that becomes that severe and systemic cannot be treated effectively with a short-term course of antibiotics.
Some doctors who may be Lyme literate–ie, who understand the complexities of the disease and its diagnosis described above–are fearful of prescribing long-term antibiotics because it goes against the IDSA rules. They are afraid they might lose their licenses. In CT, Senator Blumenthal passed a bill that allows Lyme doctors to treat at their discretion. This was a huge victory for patients who could not get the treatment they needed; I hope this kind of legislation can be passed in other states, too (or, even better, that the IDSA guidelines will be changed).
Most of the arguments I’ve heard against chronic Lyme disease make the erroneous assumption that cases that have become chronic were caught right away and treated with a standard course of antibiotics. Herein lies the problem. Cases become chronic because they go undiagnosed for too long. Therefore, I think doctors should stop arguing over whether chronic Lyme exists, and come together to figure out how to better diagnose Lyme disease at its onset, so that chronic suffering becomes moot.
3. I’ve seen more news stories about Lyme’s co-infections lately, and I know you’ve written about those recently, too. What are some the biggest misconceptions about Lyme disease and co-infections you’d like to dispel?
I am so glad to see that Lyme disease awareness is spreading, and am grateful to WBUR for their week-long coverage of the disease. I’m especially grateful that they also included co-infections in their discussions, because we can only win the battle against tick-borne illnesses if we spread awareness about all of them. Co-infections such as babesia, erhlichia and bartonella (the first being parasitic, the second two bacterial) can be transmitted from the same tick that transmits Lyme disease. They can complicate treatment, and require different medications than standard Lyme disease. Some patients with Lyme don’t get better because they are not being treated for the whole picture. I think it’s imperative that doctors who suspect Lyme in a patient also test for co-infections. A true Lyme-literate physician will also be literate in the diagnosis and treatment of co-infections. I think sometimes these infections are overlooked because they’re obscure (difficult to pronounce!) and people don’t know much about them, but that’s a grave mistake.
4. It’s summer, and here in New England the deer tick population is intense. What are some practical, everyday tips for tick prevention?
The most important thing to do is to make tick checks part of our daily routine, not just for ourselves, but for our animals, too. Taking a shower immediately upon coming in from outside is helpful, as is throwing clothes in the dryer for 20 minutes (ticks can’t survive the high heat). When hiking or camping, it’s important to wear long sleeves and light-colored clothing (to make ticks easier to see). Using bug spray with DEET is helpful, but permethrin is even better. This synthetic tick-repellent can be sprayed on shoes and clothing. Stores like REI and LLBean even sell clothes that have already been treated with permethrin (the insecticide stays active through 6 washes).
Thanks so much, Jennifer. I’m looking forward to sharing more of your story when the book comes out, and to seeing more of your published writing on chronic Lyme and Lyme’s co-infections. Keep up the good work!
If you have experiences with Lyme disease/misdiagnosis or tips to share alongside Jennifer’s, please do!
In the “before” days, I used to say that some women got babies, and I got book deals instead.
And then in an incredible and ironic twist of fortune, I got both—at the same time.
My quip became, my second book and my first baby were due on the same day. The baby came a little early, the book ended up being a little late, and they both arrived at just the right time.
That’s the short version. The long version is one I couldn’t write until now—until the final final edits were turned in and accepted, until the Table of Contents page was revised again, the book design was agreed upon, and the title was a go.
And, of course, until the regular semester was over, my summer classes had found their groove, and we’d moved out of our house. (Note: we haven’t moved into our new one yet, which is another update altogether.)
But really, it was a version I couldn’t tell until I could finally stop and just be, if even for half an hour. I hate the trite comparison that writing a book is like giving birth to a baby. Having been through both, I can vouch for the insipidness of that saying. Yet I do get stuck on the word “labor.” As in, to work, to toil, to physically strive for something.
Writing a book is not an easy task. Writing a book like my second book, a social history of modern chronic disease, which requires an extensive amount of research, interviews, and synthesis, would never have been easy. But researching it over the course of the past three years and writing it over the course of the past two? Honestly, it’s been grueling. Challenging, wonderful, exciting, and rewarding—absolutely. But finding the physical hours to carve out for it and the mental clarity and headspace to give it what it needed was one of the hardest things I’ve done.
(A quick recap of the past two years: high-risk, medically –intensive pregnancy, newborn/infant with health problems, catastrophic family illness, full-time job, teaching overload on top of that, new business, selling one house and buying another, chronic illnesses, etc., etc.)
I made a promise to myself and to my daughter that none of these other obligations would impact my time with her. I was (and am) fortunate enough to be her primary caregiver and to only use part-time childcare. That means getting everything else done around her, and that flexibility comes with a lot of choices. When you throw a book into this mix, almost everything else—socializing, blogging, sleeping—falls to the wayside.
Getting this book done was active, conscious, deliberate work. I remember setting my alarm for 4:30 am after stumbling into bed after the midnight feeding for almost a whole semester, tip-toeing in the dark past the nursery to my office, where I tried to squeeze into two hours of writing before she woke up and it was feed-play-leave for work time. There were the Thanksgivings, Christmases, Easters, Mother’s Days, and Memorial Days where I stole away with my laptop the minute my daughter went in for a nap or went to bed. Eight pm through midnight became a built-in, automatic part of my workday.
(Side note: I am extremely thankful my daughter sleeps well, and predictably.)
My husband’s new business has him working both weekend days nine months a year, so when he got home late Saturday and Sunday afternoons, we’d trade off, and my workday would begin. We made it work, because that’s what you do when it’s worth it.
For most of this time, I lived in the extremes I thought I’d moved past, the kind of mindset where the only two “sick” days I let myself take were days when my doctor had to ask me, “Are you sure you shouldn’t be in the hospital? I think I should admit you…?”
I lived this way knowing it wasn’t sustainable long-term, and that’s sort of the point. My daughter will only be young once, and I don’t want to miss anything. Time is precious and fleeting as it is, as evidenced by our current state of bike riding, sentence speaking, ladder climbing, number counting, and general big kid-ness.
Getting a deal for a book like this, especially in the current economic climate, is an opportunity for which I am acutely grateful. I had the chance to ask questions I didn’t know the answers to, and was given the time and space to try and figure them out. I had to do that opportunity justice.
Some days, when I was particularly run down, I wondered what it would be like if all of this didn’t happen at the same time, but that was the exhaustion and self-doubt creeping in. It took me longer to finish the book than I anticipated, but the book is much better for that time and space. I wandered down paths I didn’t even know to consider when I started, and those journeys made for a richer discussion.
In the end, I fought. I fought to preserve my time with my daughter, and I fought to get this book done when I often felt pulled in many other directions…because that’s what you do when it’s worth it, and because it’s worth it, there’s no choice then but to do it. Most parents out there can echo that, no matter our disparate circumstances.
I write this not as an apology for my somewhat erratic presence in this space but as an explanation. Many things had to give, and I’m starting to recalibrate things a bit—new posts, new look, new perspective…lots of changes, and more engagement.
But tonight? Tonight I’m going to leave the student papers for the morning, and power down the laptop. For the first time in so long, it’s really a Friday night.
So I am way late in writing about the now-infamous Time cover story “Are You Mom Enough?”
I’ve read lots of responses to it, including this thoughtful Boston.com blog post, but every time I tried to compose a post, life (work, infection, moving,) and, well, mothering, pulled me away. So here it is, 3:30 am, and I just finished up some work and can begin drafting my thoughts.
More than anything else, my initial reaction after reading the article on Dr. Sears and attachment parenting (and the extreme some parents can take it to) was to ask, who cares? I’m not being glib here. I am too busy getting through the day and doing the best I can for my kid and for everyone and everything else in my life to care what other mothers and families are doing. Formula or breast milk? None of my business. Pacifiers or thumb sucking? Again, not my call. What’s it to me if you co-sleep or Ferberize or Baby Whisper your way through the night? I’ve got my own sleep to worry about. I have my preferences and my data and evidence for my own decisions, and a pediatrician I trust to discuss things with, but my choices don’t need to be yours.
Before my daughter was born, I read Dr. Sears’s Baby Book. And I read What To Expect the First Year, and the American Academy of Pediatrics’ Caring For Your Child, Birth-5 Years. I read books on breastfeeding and sleep habits and baby-food making. I bought a baby carrier and pacifiers and washed the sheets for the hand-me-down bassinet.
And you know what? Then I had my daughter, and I quickly realized the best information about raising her came from her, that if we paid attention to her cues and adapted as her needs changes and listened to our instincts, we’d figure it all out.
Turns out she hardly used the bassinet because her reflux and other health problems meant she needed to be upright. Turns out she loved napping with her head on my chest and her legs tucked up under her, and that the old adage I’d read was true: Babies don’t keep, so hold them as often as you can. Focus on the moment.
Turns out she loved her pacifiers but gave them up without much fuss. Turns out she didn’t really need that 4am feed and just wanted to hang out, and that sleeping through the night came naturally for her when she wasn’t waking up to socialize. Turns out she didn’t use that baby carrier nearly as much as she did in my pregnancy daydreams because even as a tiny infant, she always wanted to be upright and on the move. Turns out my husband was right, a baby food maker is unnecessary if you have a couple of pots, a blender, and the desire.
Turns out the world didn’t end and I didn’t feel any less bonded when I had to stop breastfeeding at six months (this, after eliminating dairy, soy, and eggs; after lactation consults and digital scales and hospital grade pumps; after mastitis and supply issues and multiple supplements every day and Oh My God I am spending far too much time pumping for so few ounces when I could be spending time with my baby!) Plenty of other mothers nurse much longer, and some never do, and we’re all doing the best we can with the variables we have. The learning curve of motherhood is steep enough.
So why does this idea of “mommy wars” persist? Jenn at What The Blog?, wrote, “Mommy wars aren’t created by magazine covers. They’re created by moms who doubt their own choices then attack others who are different just because they’re threatened by self doubt. Mommy wars aren’t against each other. They’re against ourselves, and that’s why no one ever wins.”
To an extent, I agree with this. With some time and distance to move past my immediate reactions to this dialogue, and as I watch my daughter grow into more of an independent little person every day, it occurs to me that parenting is an opportunity not to be better than, but simply to bebetter: better versions of ourselves, because our children notice everything we do, because just as we take cues from them, they take so many cues from us.
If we want our children to be compassionate, to be open-minded, to be the ones who stand up for the misfit on the playground or speak respectfully to elders, that starts with how they see us treating others, speaking to and about others, and speaking to and treatingthem. If we want them to have confidence in themselves and in their ability to make decisions and act independently, then we need to model that confidence in our choices—our parenting choices, our work choices, our lifestyle choices.
Maggie May at Flux Capacitor writes, “We are given this gift in our children, the gift to be stewards of the making of their brains and souls and bodies. We are watching a supernova be born, we are watching something as breathtaking and fragile and combustible and miraculous and beautiful as a star being born in the few first years of our children’s lives.”
I am not a patient person, not naturally inclined to be carefree or completely engaged in the present. When I am with my daughter, those things come much more easily. That is a gift she gives me.
In some ways, I am in a little mothering bubble—not quite a SAHM but with an unconventional schedule that allows me lots of time with my daughter, and despite a full course load and teaching overload plus a writing career, not a traditional working mother, either. It’s hard to find a real sense of community when you straddle different worlds (a longer post on this is coming), but it also insulates me a bit from whatever competition or judging might go on (mostly).
But what I’ve taken from the newborn classes and infant music sessions and the playgrounds and library storytimes is this:
Look for the mothers who, despite the blowout diapers and missed naps and toddler meltdowns, despite the lack of sleep or downtime and the stress of the daily grind that motherhood entails, have joy. Joy in their children, joy in the visceral, physical act of parenting. I’ve seen them, I’ve witnessed their ease and confidence and comfort in their own mothering skin, and I’ve learned from them. Whatever Mommy Wars might be going on don’t seem to touch them. That is a gift they give to their children.
It’s been an intense spring, one marked by necessary cuts. Some are exciting and liberating and others are more raw, but all are ultimately for the better.
Like many of you, I suspect, I often write and blog to process, to work through decisions and reflect on experiences that have already happened. A couple of months ago, when I wrote this post that started as a rumination on the writing and editing process, it really did begin with writing itself, and slowly stretched to ideas about living with illness. Still, it was primarily retrospective.
But I thought about the idea of “necessary cuts” constantly after I posted, and a couple days later, I had a life-altering epiphany. The writing informed the decision, not vice versa.
We should sell our house and move.
A few weeks after that moment of clarity, our house was thoroughly scrubbed, streamlined, and staged, and went on the market. We scoured neighborhoods in new places, comparing schools and commutes and spaces, and driving by listings. Just a couple of weeks later, our house was under agreement, and a few weeks after that, we signed an offer on a house in a much different place.
For the past four and a half years this has been a wonderful home. It’s got character and a good layout, and is in an active area with many urban amenities: public transit, coffee shops and restaurants and playgrounds in walking distance, proximity to highways and hospitals and so much else. Yet many of the things that were attractive to us then don’t necessarily reflect our reality now. Just as suddenly as we fell in love with this place (and it was immediate—we weren’t even looking for a new house), we knew it was time to move on.
For the first time since I was eighteen, I can see myself living somewhere where espresso, Thai food, and the subway are not within steps of my door. There are many reasons to leave that make sense to us, just as there were many reasons to live here when we bought it. But this house, as much as we love it, and the lifestyle this house represents, simply aren’t the right fit for us anymore.
It’s a necessary cut, indeed.
We held our breath a lot in this house, and did a lot of hedging. We were drawn in by the spacious, quirky bedrooms, eyeing the sunny front bedroom as a possible nursery someday, yet in the same breath we told the then-sellers to take their swing set with them because we knew there was a real chance we’d never have a child to push on those swings.
We are living in the after, not the “if,” and we have a lot more clarity in terms of what we want, but more than that, what we need.
Beyond concrete items like the walk-in closet or the updated kitchen, there are many things I will miss about this house. It was where neighbors became friends. It was where a business was launched over tamales and margaritas with friends, and where Supper Clubs were held well into the night. It was the home where an idea for a second book took root, and where, over several years, the stack of books and articles somehow became a cohesive narrative. It was where we hosted Thanksgivings and cook-outs and sleepovers with nieces. Its closeness to Longwood Medical Area meant it served as a home base and staging ground whenever my loved ones (or me) were in the hospital (which was far too often, really. Really.)
Our bedroom is where I closed the door and cried quietly month after month (after month), and my home office is where I got the call that finally brought happy tears after so many years. The sunny front bedroom is where we painted the walls a gorgeous pale blue/aqua color because we wanted our little girl to have something other than pink, and on whose walls we stenciled the words “Dream. Hope. Believe,” scarcely believing this was in fact our reality.
The sunshine that streams through the living room window every afternoon was my constant companion during weeks of bedrest, and the hustle and bustle of cars, trucks, and neighbors connected me to the world outside those four walls. The front door was covered in balloons and Welcome Home signs when we brought our baby home from the hospital, and the hardwood floors and living room rug are where she crawled and walked for the first time.
We’ve had so much joy here, and so much tough stuff along with that joy. Things fell apart and stitched themselves back together—not seamless, but stronger nonetheless.
In a few weeks, we’re off to someplace much different. More land, more green, more (mental and physical) space to exhale. I did not realize how much I was still holding my breath, until I wasn’t anymore. We’re sad to leave the house was truly a home, but we’re even more excited for a better fit, a better life for all of us.
I’ve been pretty quiet lately. I have some updates I’ll post later this week, but today seemed like a great day to look at (Weekly) Grace in Small Things.
–My husband had to work today, so it was just my daughter and me. We did our usual morning eat-play-dress routine, and as we headed out to go to church and to do some visiting, the sun broke through the clouds and “My Girl” came on the radio. What more could a Mama ask for on Mother’s Day, really?
–Every stage is so much fun, but I particularly love the constant narration of daily activity phase we’re in right now. “I did it!” she says, standing up with a huge grin on her face after she completes a task. “All done now. Bye-bye!” she says, shoving her plate of food away from her. “I’m all set,” she says as she’s buckled into her car seat.
–Watching my daughter and all of her grandparents interact and seeing how much they love each other is great to witness. One of my favorite little things? When my daughter walks over to me with the phone in her hand, hits speaker and re-dial, and calls my mother to ask her to sing “Ba Ba Black Sheep.” Asking her who loves her and hearing her say their names? Amazing.
–I want my daughter to feel like part of a pack and that she is loved by and connected to more than just her father and me. She loves her eight cousins and when she asks for them by name, it takes me down the road a few years to sleepovers and bike rides and those all-important bonds you have with the people who have known you your entire life. She woke up and asked to call some of her cousins today. While I wouldn’t oblige her since it was 6:30am, it did make me smile.
–Lately, she likes to take both my cheeks in her hands and kiss my face noisily and earnestly. It makes me laugh, which makes her squeal with laughter and eggs her on, which makes her lean in and kiss me again with even more exaggeration, which makes both of us laugh harder. We just went through several rounds of this before bedtime. It doesn’t do much to settle her down, admittedly, but it’s hilarious and I know she’ll move on to something else soon enough; I don’t need to rush that.
Nineteen months into this, I still can’t believe I get to be someone’s mother, that I get to be her mother. She lights up corners of our world we didn’t even know existed.
Happy Mother’s Day to all the women who love, nurture, guide, and advocate for children out there.
(And, back to regularly scheduled posts this week. Promise.)
Amoxil (amoxicillin) is a widely used prescription antibiotic from the beta-lactam penicillin family. It is commonly prescribed for infections of the ears, throat, lungs, urinary tract, skin and stomach. This guide explains in clear language how Amoxil works, what it is used for, how to take it safely, and what to consider if you are looking for an Amoxil amoxicillin online purchase.
Amoxil is the brand name for amoxicillin, a semi-synthetic broad-spectrum antibiotic. It belongs to the pharmacotherapeutic group of beta-lactam antibiotics, specifically the subgroup of broad-spectrum penicillins known as aminopenicillins. The active ingredient in Amoxil is amoxicillin, which is designed to be stable in the acidic environment of the stomach so it can be taken by mouth and still be well absorbed.
Because of its reliable activity against many common bacteria and its generally good tolerability, Amoxil is frequently one of the first-line antibiotics prescribed for everyday infections such as middle ear infections in children, strep throat, sinus infections, bronchitis, urinary tract infections and certain stomach infections associated with Helicobacter pylori. When used correctly and only when truly needed, it can be a very effective and safe treatment option.
How Amoxil Works in the Body
To understand Amoxil, it is helpful to know the basics of how bacteria live and grow. Bacterial cells are surrounded by a firm outer structure called the cell wall. This wall gives the bacteria its shape and protects it from the outside environment. Amoxil interferes with the formation of this cell wall. It blocks specific enzymes (called transpeptidases or penicillin-binding proteins) that are needed to build the wall’s backbone, known as peptidoglycan.
When these enzymes are blocked, the bacterial cell wall becomes weak and unstable. Water can then flow into the bacterial cell, causing it to swell and eventually burst in a process called osmotic lysis. Because Amoxil actively kills bacteria in this way rather than simply stopping them from multiplying, it is described as a bactericidal antibiotic. It is most effective against bacteria that are actively growing and dividing, which is why it is important to take each dose on schedule to maintain steady levels of the drug in the body.
Bacteria Amoxil Can and Cannot Treat
Amoxil has a broad spectrum of activity. This means it can act against many different types of bacteria, including both Gram-positive and Gram-negative species, as well as some anaerobic bacteria. However, no antibiotic works against all germs, and Amoxil is ineffective against viruses such as those that cause the common cold or flu.
Typical bacteria that Amoxil can treat include:
Gram-positive aerobes such as Streptococcus species (including S. pyogenes, S. agalactiae, and S. bovis), Enterococcus faecalis, Listeria monocytogenes, and some strains of Corynebacterium diphtheriae that do not produce beta-lactamase.
Gram-negative aerobes such as Haemophilus influenzae, Haemophilus parainfluenzae, Moraxella catarrhalis, many strains of Escherichia coli, Proteus mirabilis, and Helicobacter pylori.
Anaerobes including Peptostreptococcus species and some Clostridium species that do not produce beta-lactamase.
Other organisms such as Borrelia burgdorferi, the bacterium responsible for Lyme disease.
Bacteria that Amoxil does not work well against include:
Staphylococcus aureus strains that produce beta-lactamase (these enzymes can break down amoxicillin).
Certain Gram-negative bacteria such as Enterobacter species, Klebsiella species, Pseudomonas aeruginosa, and Acinetobacter species.
Organisms without cell walls like Mycoplasma species, or those that live inside cells like Chlamydia, Rickettsia, and Legionella.
Resistance to Amoxil can develop. Bacteria may produce enzymes called beta-lactamases that break down the antibiotic, change the structure of the penicillin-binding proteins so the drug can no longer attach, or reduce the ability of the drug to enter the bacterial cell. This is one reason why it is vital to use Amoxil only when prescribed and to complete the full course of treatment.
How Amoxil is Absorbed and Eliminated
After an oral dose, Amoxil is absorbed quickly and almost completely from the digestive tract. Up to about 95% of the dose can be taken up, and the bioavailability – the amount that actually reaches the bloodstream – is typically between 75% and 90%. Food has very little effect on absorption, so Amoxil can be taken with or without meals.
The highest concentration in the blood (known as Cmax) is usually reached about 1–2 hours after taking a 500 mg dose, with typical levels around 6–11 micrograms per millilitre. Only a small portion (around 17–20%) of the drug is bound to blood proteins, which allows it to spread widely throughout the body. Amoxil penetrates well into many tissues and body fluids, including the mucous membranes of the airways, sputum, bile, bone tissue and peritoneal fluid. It crosses into the fluid surrounding the brain and spinal cord only to a limited degree under normal conditions, but concentrations increase during meningitis.
Amoxil is broken down only partly in the body into inactive substances. Most of the active drug is removed by the kidneys. Around 60–80% of a dose is excreted unchanged in the urine within about six hours. The typical half-life – the time it takes for the concentration in the blood to fall by half – is about 1–1.5 hours in people with normal kidney function, but it can be prolonged up to roughly 8.5 hours in severe kidney failure (anuria). Because of this, people with reduced kidney function often need dose adjustments or longer intervals between doses.
Conditions Treated with Amoxil
Amoxil is prescribed for infectious and inflammatory diseases caused by bacteria that are known, or strongly suspected, to be sensitive to amoxicillin. Common indications include:
Upper respiratory tract infections: such as tonsillitis, pharyngitis and sinusitis, as well as middle ear infections (otitis media). These are frequent in both children and adults.
Lower respiratory tract infections: such as acute bronchitis and certain forms of pneumonia, often as part of a combination regimen if multiple bacteria are involved.
Urinary tract infections (UTIs): including cystitis, pyelonephritis and urethritis, provided the causative organisms are susceptible.
Gastrointestinal infections: such as gastritis and peptic ulcer disease associated with H. pylori, where Amoxil is typically combined with other antibiotics and acid-suppressing medications as part of an eradication protocol.
Skin and soft tissue infections: including abscesses, furunculosis (boils) and erysipelas.
Other indications: such as Lyme borreliosis (Lyme disease), prevention of bacterial endocarditis in high-risk patients undergoing certain procedures, and some infections of the biliary tract.
Even if these conditions sound familiar, self-diagnosing and self-treating with antibiotics is risky. A healthcare professional should confirm that an infection is present and choose the right antibiotic and dose based on your medical history, allergies and local resistance patterns.
Who Should Not Take Amoxil
Amoxil is not suitable for everyone. You should not take this medication if any of the following apply to you:
Allergy or hypersensitivity to amoxicillin, other penicillins, or any other beta-lactam antibiotics such as cephalosporins, carbapenems or monobactams. Severe reactions can include anaphylaxis, which is life-threatening.
Infectious mononucleosis or certain blood cancers such as lymphocytic leukemia, as there is a particularly high risk of developing a widespread skin rash (exanthema).
History of severe anaphylactic reactions to any medication, especially antibiotics in the same family.
Severe kidney failure when it is not possible to reduce the dose or extend the dosing intervals appropriately.
If you are unsure whether you have ever reacted badly to penicillin or related drugs, discuss this carefully with your doctor or pharmacist before you start Amoxil, especially if you are considering an Amoxil amoxicillin online purchase where your full medical record may not be reviewed in detail.
Special Precautions and Monitoring
Even when Amoxil is appropriate, some precautions are essential to reduce the risk of side effects and complications:
Allergic reactions: Amoxil can cause reactions ranging from mild rashes to severe anaphylactic shock. At the first signs of hives, swelling of the face or throat, difficulty breathing, dizziness or rapid heartbeat, treatment must be stopped immediately and emergency care sought.
Severe diarrhea and pseudomembranous colitis: Antibiotics can sometimes disrupt the normal gut flora, allowing overgrowth of harmful bacteria such as Clostridioides difficile. If you develop significant or persistent diarrhea, especially with cramps or blood in the stool, stop taking Amoxil and contact a doctor. Do not use over-the-counter anti-diarrheal medications unless advised, as they can worsen some antibiotic-related colitis.
Crystalluria (crystals in the urine): Very rarely, crystals of amoxicillin can form in the urine, especially when high doses are taken and fluid intake is low. To minimize this risk, drink plenty of water throughout the day.
Patients with kidney impairment: Reduced kidney function slows the removal of Amoxil from the body. In such cases, the dose or the interval between doses must be adjusted. Always inform your prescriber about any kidney disease or a history of kidney problems.
Jarisch–Herxheimer reaction: During treatment of Lyme disease caused by Borrelia burgdorferi, some patients experience a short-lived worsening of symptoms such as fever, chills and muscle pain within the first days of treatment. This is called a Jarisch–Herxheimer reaction and is caused by the rapid killing of bacteria and the resulting release of bacterial components into the bloodstream. It usually settles on its own but should still be discussed with your doctor.
Long-term therapy: When Amoxil is used for longer periods, regular monitoring of liver function tests, kidney function and blood counts (the hematopoietic system) every 2–4 weeks is recommended.
Use in children: Amoxil is widely used in paediatrics. However, prolonged use can in rare cases lead to discoloration of tooth enamel. Good oral hygiene and regular dental check-ups are important.
Important Drug and Alcohol Interactions
Amoxil can interact with other medications, affecting either its activity or the way the other drug behaves in your body. Always provide a full list of your prescriptions, over-the-counter medicines and supplements to the prescriber and pharmacist. Key interactions include:
Probenecid, phenylbutazone, acetylsalicylic acid (aspirin) and sulfinpyrazone: these medicines can reduce the renal excretion of amoxicillin, leading to higher and more prolonged levels in the blood. In some cases this is used intentionally, but it may also increase the risk of side effects.
Bacteriostatic antibiotics such as tetracyclines, macrolides (for example azithromycin or clarithromycin) and chloramphenicol may counteract the bactericidal activity of Amoxil when used at the same time. Your doctor will consider whether combination therapy is appropriate.
Aminoglycosides: when used together with Amoxil there may be a useful synergistic effect against certain bacteria, but the drugs must be given by separate routes or at different times because they can inactivate each other when mixed directly.
Oral anticoagulants: Amoxil may prolong prothrombin time or increase the INR (a measure of blood clotting). If you are taking medicines such as warfarin, you may need more frequent blood tests and possible dose adjustments.
Alcohol: although there is no strict “forbidden” interaction, alcohol is not recommended during Amoxil therapy. Alcohol can increase the burden on the liver, worsen side effects such as dizziness or stomach upset, and may raise the risk of allergic or toxic reactions.
Overdose: Symptoms and What To Do
Taking more Amoxil than prescribed can lead to an overdose. The most common symptoms are nausea, vomiting and diarrhea, which can cause dehydration and disturbance of the body’s fluid and electrolyte balance. Very high doses, especially in people with kidney problems, may increase the risk of seizures or kidney-related side effects.
If an overdose is suspected, seek medical help immediately. Treatment usually includes gastric lavage (stomach pumping) if the overdose is very recent, administration of activated charcoal to bind any remaining drug in the digestive tract, and symptomatic care such as intravenous fluids and correction of electrolyte abnormalities. In severe cases, especially with marked kidney impairment, hemodialysis can help remove amoxicillin from the bloodstream.
Amoxil (Amoxicillin) Online Purchase: Safety Tips
The internet has made it possible to buy Amoxil (amoxicillin) online from a variety of pharmacies and marketplaces. While this can be convenient and may reduce costs, it also carries important safety considerations. Not all online vendors follow proper regulations, and some may sell counterfeit, expired or improperly stored medicines.
If you are considering an Amoxil amoxicillin online purchase, keep the following in mind:
Prefer pharmacies that require a valid prescription and offer access to a licensed healthcare professional who can answer questions.
Check that the website displays a physical address and contact information and is licensed or accredited according to your country’s regulations.
Be wary of sites that offer unusually low prices, promise to cure every infection or guarantee “no side effects”. These are common warning signs of illegitimate sellers.
Ensure that the product details (strength, dosage form, manufacturer, expiry date) are clearly stated and that packaging is sealed and intact on arrival.
Never change the prescribed dose or duration of treatment just because you have easy online access to extra tablets. Misuse of antibiotics fuels bacterial resistance and can harm your health.
Buying medication over the internet may be economical and convenient, but it should never replace a proper medical assessment. If you develop new symptoms, side effects or your infection does not improve, contact a healthcare provider promptly.
General Prescribing and Dosing Guidelines
Amoxil is usually taken by mouth, with a glass of water. Because food does not significantly affect its absorption, doses can be taken with or without meals. To maintain stable antibiotic levels in the bloodstream, doses are typically spaced evenly through the day.
The exact dosing regimen is individualized. Doctors consider several factors, including:
the site and severity of the infection;
the susceptibility of the likely or known bacteria;
the patient’s kidney function and overall health;
the patient’s age and body weight, especially in children.
Short courses are often sufficient for uncomplicated infections, whereas more serious or deep-seated infections may require longer treatment. If long-term therapy is needed, periodic monitoring of liver, kidney and blood function every 2–4 weeks helps ensure that the drug remains safe for continued use. It is important not to stop Amoxil early just because you start feeling better; doing so can allow some bacteria to survive and potentially become resistant.
Dosage Forms and Storage Conditions
Amoxil is available in several oral dosage forms, making it suitable for adults and children:
film-coated tablets containing 250 mg, 500 mg or 1000 mg of amoxicillin;
hard gelatin capsules with different strengths of amoxicillin;
in some markets, oral suspensions or dispersible tablets for children or people who have difficulty swallowing tablets.
Tablets and capsules should typically be stored at temperatures below 25 °C, in a dry place protected from moisture and direct light. Keep all medicines out of the reach of children. The usual shelf life ranges from 2 to 4 years depending on the specific dosage form and manufacturer. Do not use Amoxil past the expiry date printed on the package and return unused or expired medicines to a pharmacy for safe disposal.
When used correctly, Amoxil can be a powerful tool against many common bacterial infections. Thoughtful use, medical supervision and cautious approaches to Amoxil amoxicillin online purchase will help ensure that treatment is both effective and safe.
Ciprofloxacin, commonly known by the brand name Cipro, is a widely used prescription antibiotic from the fluoroquinolone class. It is designed to fight a broad range of bacterial infections and is often considered when other antibiotics are not suitable or have not worked. Understanding how Cipro works, when it is prescribed, and how to use it correctly is essential, especially for people who are exploring options to buy Cipro online OTC through licensed internet pharmacies.
Ciprofloxacin is an International Nonproprietary Name (INN) antibiotic that belongs to the second generation of fluoroquinolones. It is a synthetic, broad-spectrum antibacterial medicine that acts against many types of gram-positive and gram-negative bacteria. In simple terms, it is designed to kill a wide range of harmful bacteria that can cause infections in the lungs, urinary tract, digestive system, skin, bones, and other parts of the body.
Under the brand name Cipro, this medicine is commonly supplied as film-coated tablets in different strengths. The active ingredient in a standard 500 mg tablet is ciprofloxacin, usually in the form of ciprofloxacin hydrochloride monohydrate. People searching for Cipro buy online OTC are usually looking for a convenient way to access these tablets for conditions previously diagnosed by a healthcare professional.
Ciprofloxacin is not effective against viruses, such as those that cause the common cold, influenza, or most sore throats. It should only be used when a bacterial infection has been confirmed or strongly suspected by a doctor. Because of the strength and broad activity of this medicine, responsible use is very important to protect your health and to reduce the risk of bacteria becoming resistant to treatment over time.
Composition and Form of Cipro Tablets
Each Cipro tablet contains the active substance ciprofloxacin hydrochloride monohydrate, which corresponds to a specific amount of ciprofloxacin (for example, 500 mg of ciprofloxacin per tablet). In addition to the active ingredient, several inactive substances, or excipients, are used to give the tablet its shape, stability, and appearance.
Typical excipients found in Cipro tablets may include corn starch, pregelatinized starch, crospovidone, lactose monohydrate, microcrystalline cellulose, talc, and magnesium stearate. The outer shell or coating often contains polymers such as hypromellose and copovidone, as well as macrogol-4000, propylene glycol, talc, and titanium dioxide to create a smooth, easy-to-swallow tablet with a consistent appearance.
These inactive ingredients generally do not affect the antibacterial action of the drug, but they can be important for people with specific allergies or intolerances (for example, lactose intolerance). If you have known sensitivities, always review the full composition in the official instructions or consult your doctor or pharmacist before you buy Cipro online OTC from any source.
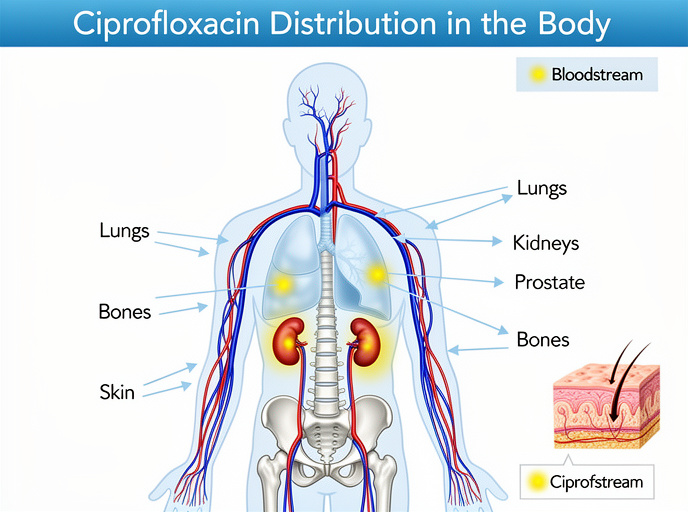
A simplified view of how ciprofloxacin circulates to different organs after oral intake.
How Cipro Works: Mechanism of Action
Ciprofloxacin works by targeting important bacterial enzymes called DNA gyrase (topoisomerase II) and topoisomerase IV. These enzymes are essential for bacteria to copy and repair their genetic material (DNA). When ciprofloxacin blocks these enzymes, the bacterial cells can no longer divide and repair themselves normally. As a result, the bacteria die rather than simply stop growing.
This type of action is called a bactericidal effect, meaning that the drug actively kills the microorganism instead of just slowing it down. Because of this mechanism, Cipro can be very effective in treating serious infections when used correctly and at the right dose for a sufficient length of time.
However, this strong effect also means that Cipro must be used with caution. It should not be taken for minor or self-limiting illnesses that are likely to be viral, and it should always be used according to medical advice. If you are considering options to Cipro buy online OTC, it is important to base that decision on a prior diagnosis and treatment plan provided by a licensed healthcare professional.
When is Cipro Prescribed?
Ciprofloxacin is prescribed for a wide variety of infections caused by bacteria that are sensitive to it. These may include infections of the respiratory tract, urinary tract, digestive system, skin, soft tissues, bones, joints, and certain systemic infections. Doctors usually decide to use Cipro when laboratory tests or clinical experience suggest that the likely bacteria will respond well to this medicine.
Examples of conditions where Cipro may be used include:
Lower respiratory tract infections such as pneumonia (often as part of combination therapy with other medicines) and exacerbations of chronic bronchitis.
Upper respiratory tract infections like sinusitis, including maxillary sinusitis, in cases where bacteria susceptible to ciprofloxacin are identified.
Ear infections such as otitis media when caused by susceptible organisms.
Urinary tract infections (UTIs), including cystitis, pyelonephritis, and urethritis.
Prostatitis, as ciprofloxacin tends to penetrate well into prostate tissue and can help clear infections more effectively.
Certain sexually transmitted infections such as uncomplicated gonorrhea, depending on local resistance patterns and clinical guidelines.
Intra-abdominal infections such as peritonitis and biliary tract infections.
Bacterial diarrhea and gastrointestinal infections including salmonellosis, shigellosis, and infections caused by some strains of E. coli.
Skin and soft tissue infections such as furunculosis, abscesses, and infected wounds.
Bone and joint infections like osteomyelitis.
Prevention and treatment of anthrax, including inhalational exposure to Bacillus anthracis, under strict medical supervision.
Ciprofloxacin is not used for viral infections such as the flu or routine colds. It is also not recommended for preventive use unless there is a clear risk of bacterial infection documented by medical evaluation. Even if you can buy Cipro online OTC, it should never replace professional medical assessment.
Bacterial Resistance to Cipro
Like all antibiotics, ciprofloxacin can become less effective over time if it is misused or overused. Bacteria can develop resistance through several mechanisms. Some bacteria undergo genetic mutations that change the structure of DNA gyrase or topoisomerase IV, making it harder for Cipro to bind to these targets. Others may reduce the permeability of their cell membrane or actively pump the drug out of the cell using so-called efflux systems.
These adaptations mean that the bacteria are no longer killed by normal doses of the medicine. Although cross-resistance between fluoroquinolones and other antibiotic families (such as macrolides or beta-lactams) is usually limited, resistance to Cipro still reduces valuable treatment options. To slow down the development of resistance, you should only take ciprofloxacin when it is truly needed, at the dose prescribed, and for the full duration recommended by your doctor.
Stopping treatment early because you feel better or using leftover tablets later for a different illness both increase the risk of resistance. This is especially important for people who buy Cipro online OTC, since self-directed treatment without clear guidance may lead to incorrect dosing and incomplete courses.
How Cipro Behaves in the Body (Pharmacokinetics)
After you swallow a Cipro tablet, the active ingredient is absorbed from the digestive tract into the bloodstream. The oral bioavailability of ciprofloxacin is roughly 70%, which means that a significant portion of the dose reaches your circulation. The highest blood concentration is typically reached within 1 to 2 hours.
Once in the bloodstream, ciprofloxacin distributes into many tissues, including the lungs, kidneys, prostate, bones, and skin. This good tissue penetration helps explain why Cipro can be used for such a wide range of infections. The drug is partially metabolized in the liver and then eliminated mainly through the kidneys in the urine, and to a lesser degree through bile and feces.
The half-life of ciprofloxacin in adults is usually between 4 and 6 hours. This is the time required for the concentration of the drug in the body to fall by half. The half-life influences how often the medicine needs to be taken each day. In many cases, Cipro is prescribed once or twice a day, but the exact dosing schedule depends on the type and severity of the infection, kidney function, and other individual factors.
In people with reduced kidney function, ciprofloxacin may stay in the body longer, so dose adjustments are often needed. This is another reason why a medical evaluation is important before you decide to buy Cipro online OTC. Your healthcare provider can interpret blood tests, kidney function, and other health factors to choose the most suitable dose and dosing interval.
Who Should Not Take Cipro (Contraindications)
Ciprofloxacin is not suitable for everyone. Certain conditions and risk factors mean that the medicine should be avoided or only used under very strict supervision. You should not take Cipro if you have a known allergy or hypersensitivity to ciprofloxacin, other fluoroquinolones, or any of the excipients in the tablet.
In general, Cipro is contraindicated during pregnancy and breastfeeding because of potential effects on the developing child. It is also not routinely used in people under 18 years of age, except in special situations such as children with cystic fibrosis or for the prevention or treatment of inhalational anthrax when no safer alternatives are available.
Ciprofloxacin should also not be used in people with a history of certain neurological conditions such as epilepsy or other seizure disorders, severe diseases of the central nervous system, or in patients with myasthenia gravis, a disease that leads to muscle weakness. In these individuals, Cipro may worsen symptoms or increase the risk of serious side effects.
There are also situations where Cipro must be used with particular caution. These include patients with cerebrovascular atherosclerosis, severe kidney or liver impairment, pre-existing heart rhythm disturbances, depression, or other mental health disorders. In all of these cases, your doctor will balance the potential benefits and risks before deciding whether ciprofloxacin is appropriate.
Dosage and Duration of Treatment
The exact dose and length of therapy with Cipro must always be determined by a healthcare professional. Factors such as the location and severity of the infection, the specific bacteria involved, kidney function, age, and accompanying illnesses all influence the chosen regimen. Never adjust the dose on your own, even if you obtained the medicine through a trusted service that allows you to Cipro buy online OTC.
Typical treatment courses may include:
Uncomplicated urinary tract infections and some cases of cystitis or gonorrhea: 250–500 mg once or once daily, depending on the clinical situation and local guidelines.
Pyelonephritis and more complicated urinary or gastrointestinal infections: 500 mg twice daily for around 7 days, adjusted by the prescriber.
Respiratory tract infections such as pneumonia or bronchitis, and skin or soft tissue infections: 500–750 mg twice daily, usually for 7–14 days.
Bone infections like osteomyelitis: treatment may last up to 2 months or longer, depending on response.
Infections caused by certain organisms such as Streptococcus or Chlamydia: courses of at least 10 days are usually recommended.
It is essential to complete the entire prescribed course, even if symptoms improve earlier. Stopping too soon can allow some bacteria to survive and potentially become more resistant, which may lead to a relapse of infection and make future treatment more difficult.
Possible Side Effects of Cipro
Like all medications, Cipro can cause side effects, although not everyone experiences them. Many side effects are mild and temporary, but some can be serious and require immediate medical attention. Understanding these reactions helps you know when to continue treatment and when to seek help.
Commonly reported side effects may include:
Digestive symptoms such as nausea, diarrhea, abdominal pain, or discomfort.
Nervous system symptoms including headache, dizziness, or difficulty sleeping (insomnia).
Increased sensitivity of the skin to sunlight (photosensitivity), which can lead to sunburn more easily.
Temporary changes in liver or kidney function tests observed on blood work.
Allergic skin reactions such as rash or itching.
Heart rhythm disturbances in people who already have heart rhythm problems or are taking certain other medicines.
Rare but serious side effects: Fluoroquinolones, including Cipro, have been associated with inflammation or rupture of tendons, especially in older adults and in people taking corticosteroids. Tendon pain, swelling, or sudden difficulty moving a joint can signal tendonitis or tendon rupture. If this happens, stop taking the medicine and seek medical advice immediately.
Because of the possibility of these reactions, it is essential to read the official patient leaflet that comes with the medication and to speak with your doctor or pharmacist before and during treatment, particularly if you have other health conditions or take multiple medications.
Practical Safety Tips While Taking Cipro
To get the most benefit from Cipro while reducing the risk of unwanted effects, a few practical rules are helpful. These tips are especially important for people who use online services to obtain their medicines and may not see a pharmacist in person every time they refill their prescription.
During treatment with Cipro:
Avoid exposure to direct, intense sunlight or tanning beds. Wear protective clothing and use sunscreen if you need to be outdoors, as photosensitivity reactions can occur.
Do not drink alcohol during the course of therapy. Alcohol may increase certain side effects and make it harder to judge how the medicine is affecting you.
Avoid taking Cipro at the same time as antacids or supplements containing aluminum, magnesium, iron, or zinc. These substances can bind to ciprofloxacin in the stomach and significantly reduce its absorption. If you need these products, take them at least a few hours apart from Cipro.
Pay attention to any new tendon pain, especially in the Achilles tendon, shoulders, or hands. If pain develops, stop taking the medicine and contact a doctor immediately.
Drink plenty of fluids throughout the day to support kidney function and help the body process and eliminate the drug.
Following these measures, along with the dosing instructions from your healthcare provider, helps keep treatment effective and safer, whether you received the medicine locally or chose to Cipro buy online OTC from a reputable pharmacy.
Storage and Handling of Cipro
Proper storage of Cipro tablets helps protect their quality and effectiveness until the expiration date. In general, Cipro should be kept at a temperature not exceeding 25 °C (77 °F), away from excessive heat, moisture, and direct light. A closed cupboard at room temperature is usually ideal.
Always store the medicine in its original packaging, out of the sight and reach of children and pets. Do not use tablets after the expiry date printed on the pack, which is typically between 2 and 4 years from the date of manufacture, depending on the manufacturer. If you have leftover tablets after completing a course, do not throw them directly into household waste or wastewater; instead, ask a pharmacist about safe disposal methods.
How to Safely Cipro Buy Online OTC
Many people are interested in the possibility of Cipro buy online OTC because it can be convenient, discreet, and sometimes more affordable than traditional pharmacies. However, antibiotic treatment should never be taken lightly. To stay safe, it is crucial to combine the convenience of an online pharmacy with responsible medical guidance.
Before ordering Cipro online, you should ideally have a confirmed diagnosis from a healthcare professional and a clear treatment plan that specifies the dose and duration. When choosing an online pharmacy, look for signs of reliability such as secure payment methods, transparent contact information, clear privacy policies, and access to licensed pharmacists or medical consultation. Avoid websites that offer ciprofloxacin without any medical questions, or that promote unrealistic claims.
Compare available tablet strengths (for example 250 mg, 500 mg, 750 mg, or 1000 mg) and select pack sizes that match your prescribed treatment course so you can complete the full regimen without interruption. Review shipping conditions, delivery times, and costs, especially if you need the medicine urgently. Finally, always check that the packaging you receive is intact, properly labeled, and within the expiry date. If something appears suspicious, do not start the treatment and seek professional advice.
Used in this careful and informed way, online services can complement traditional healthcare by making it easier for patients to access the medication they need, while still respecting medical guidelines and antibiotic stewardship principles.
The last conversation we had with my grandmother began like this:
“It’s Easter! Have you eaten yet for the holiday?” We had to strain to hear her through the oxygen mask over her face, but she was not deterred by that, or by the extreme stress her heart and lungs were under.
If you knew my Nana, you would not be surprised this was the first thing she said when she opened her eyes and saw us gathered around her hospital bed. The consummate Italian cook and family matriarch, she considered feeding her family the ultimate act of love, of physical and emotional nourishment.
To say her death at 92 was truly a shock is a testament to the indomitable force of nature she was, a feisty, active, sharp, loving, funny, tenacious, and hardworking woman until the very end. If you knew my Nana, you knew how relentless she could be in pursuit of what she believed, how dogged she could be in her role as devoted wife, mother, grandmother, or great-grandmother. Your shoulders would shake with laughter and your eyes would tear a bit as you recounted her latest wild escapade, or heard the most recent “Nana-ism.”
A force of nature, indeed.
Those of us who know her have all these stories, we catalog them and re-tell them and they are our buffer from the reality of grief, our collective place to land. As one writer likened it, they are our pockets full of gold.
So while I keep them preserved among those who know them and know her best, here’s what I know.
I know she lived, as my husband said, a big life—one filled with sacrifice and sorrow, unquestionably, but one filled with so many relationships, so much love and grace.
I know from every handwritten note or pot of tomato sauce, from every Rosary she prayed for us, or wacky Christmas gift we received, that we were loved. I also know she knew how much she was loved by her family.
We ended every phone call with “I love you.” Two days before she died, I got to hear my daughter say “I love you, Nana” and got to see my Nana’s reaction to it. I know that makes me incredibly fortunate.
The last interaction we had while she was awake was when I held her hand and then kissed it. No words were exchanged in that moment, but she felt it, and it said everything we needed it to.
I know I miss her already.
I know that when I shake my head, smiling, and use the word “relentless” in relation to my daughter’s quest for whatever object or task she is focused on, that I am seeing shades of my grandmother in her.
I know that what I want for our daughter is a big life, too.
While saving a podcast I created for my students the other day, I inadvertently clicked on another item in my iTunes folder: my daughter’s first cry, recorded with my husband’s iPhone the moment she was born.
Momentarily overwhelmed with emotion, I scrolled through until I found another amazing entry: the sound of her hiccupping in utero, recorded with my iPhone during one of the many non-stress tests I had during my pregnancy. You hear the whoosh and thump of her heartbeat, and then every few seconds, you hear this unmistakable blip that is a hiccup.
An entry from a few months later makes my body clench: the horrifying sound of her struggling to breathe, rasping and gasping and choking and wheezing, when she was quite sick as a young infant. I played it for her new specialist so he could see what I meant when I talked about how much she struggled at night and while eating.
He nodded, playing it over several times, and sharing it with the fellow on his rotation. “I am so glad you recorded this,” he said to me, relaying any private fears of mine I’d look like some overly paranoid first-time mother. It was the first step in accurately identifying some of her health problems and getting her the right treatment.
My smart phone is just one of many ways technology has changed my experience of being a patient, being a pregnant patient, and being the mother of a patient. I get text messages from my pharmacy when it’s time to refill my prescription, and can accomplish more over brief e-mail exchanges with my own specialist than I do in some office visits. The patient health management platform my hospital uses has all lab results, imaging, results letters, and medical history available with a few clicks on a password-protected site.
I’ve written here before how social media is an important—and often, the only—source for connecting with other rare disease patients, people who can provide the anecdotal information on treatments and best practices that can make such a difference, information that we can use to have conversations with our physicians. It’s another form of data, and in the digital world of health information, data matters more and more.
I’ve been writing and researching in a lot more depth the way technology and social media have influenced patient-hood, and I know this post is just a snapshot glimpse of the many, many types of application. But as someone immersed in the research and the statistics, what I would really love to hear more about are the everyday experiences people have.
So tell me, how do you use technology to manage illness? How have technology and social media influenced your experiences as a patient? How you advocate for yourself or find information?